|
 |
||||||||||||||
|
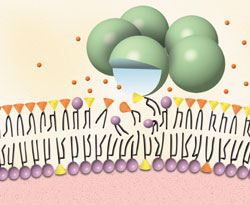
C-reactive protein (CRP) is a nonglycosylated polymeric protein consisting of five identical subunits. It is found in most vertebrate species, and is well conserved biologically throughout evolution.1 It has been identified in the horseshoe crab, an arthropod that is some 500 million years old. CRP is one of the "acute phase reactants," i.e., proteins that are produced by the liver to combat the invasion of foreign antigens. CRP was discovered in 1930 when it was shown that it could bind to pneumococcal C polysaccharide. It is now known that CRP specifically recognizes phosphocholine, the hydrophilic portion of phosphatidylcholine, in cell membranes (Figure 1). Complexation of CRP to the cell wall activates complement via the classical pathway, and stimulates macrophages and other cells to undergo phagocytosis. Figure 1. The structure of CRP and its binding to the cell membrane. Reproduced with permission. The reference range of CRP is 0 to 1.0 mg/dL. In patients with acute inflammation, the concentration can increase 1000-fold. In contrast, other acute phase reactants such as fibrinogen, haptoglobin, ceruloplasmin, and complement proteins C3 and C4 increase only two- to threefold or less, relative to baseline concentrations. Release of CRP is mediated by cytokines such as interleukin-6, which stimulate hepatocytes to preferentially produce positive acute phase proteins in lieu of other negative acute phase proteins (such as albumin and transferrin).2 High concentrations are observed in patients with infections, malignancies, stress, arthritis, trauma, surgery, and acute myocardial infarction (AMI). CRP
in cardiovascular disease CRP
for cardiovascular risk among healthy subjects
Figure 2.
Measurement of CRP for risk stratification in healthy subjects requires the individual to be free of any acute or chronic disease that might increase the baseline serum concentration of CRP. Moreover, ultrasensitive CRP assays must be used to distinguish minor increases from the upper limit of normal. CRP
in unstable angina Inflammation has also been implicated as an important initiating step in the pathogenesis of unstable angina (UA) and AMI. Infiltration of monocytes, macrophages and T-lymphocytes produce metalloproteinases which degrade the fibrous cap that normally protects atherosclerotic lesions from rupturing. Thinning of the cap makes the plaque vulnerable to rupture. As such, investigators have examined the potential role of CRP for risk stratification. Two studies of 140 and 195 UA patients using in-hospital death and AMI as endpoints showed that CRP was, in fact, not predictive.6,7 Cardiac troponin I was instead found to be useful (OR: 3.8) in one of these studies.7 However, in studies where the observation period was extended to a period of time after the patient was discharged from the hospital, CRP was shown to be predictive of untoward cardiac events. Morrow et al. reported that CRP was equivalent to cardiac troponin for predicting cardiovascular events at 14 days of follow-up, with ORs of 3.6 and 3.0, respectively.8 After 3 months of follow-up, the predictive value for CRP and cardiac troponin were even higher, as might be expected (OR: 7.6 and 10, respectively).9 Because CRP and cardiac troponin detect different steps of the pathophysiology of acute coronary syndromes, the combination of the two tests may produce more accurate predictions of future risks. CRP
following acute myocardial infarction Clinical studies have been conducted to determine a potential role of CRP following AMI. Tommasi et al. calculated an OR of 3.55 for cardiac events (death, new-onset angina, recurrent AMI) after 13 ± 4 months' follow-up of 64 AMI patients, using a cutoff of 2.55 mg/dL.11 Using a cutoff of 20 mg/dL for CRP, Anzai et al. calculated respective ORs of 4.72, 2.11, and 3.44 for cardiac rupture, left ventricular aneurysmal formation, and one-year cardiac death among 220 patients with a first Q-wave AMI.12 A summary of these and other findings is shown in Table 1. Table 1. Use of CRP after acute myocardial infarction.
DPC
IMMULITE® C-Reactive Protein assay References 1. Ballou SP, Kushner I. C-reactive protein and the acute phase response. Adv Intern Med 1992;37:313-36. 2. Kushner I. C-reactive protein and the acute-phase response. Hosp Pract 1990;25(3A):13-28. 3. Kuller LH, Tracy RP, Shaten J, Meilahn EN for the MRFIT Research Group. Relation of C-reactive protein and coronary heart disease in the MRFIT nested case-control study. Am J Epidemiol 1996;114:537-47. 4. Ridker PM, Cushman C, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997;336:973-9. 5. Olatidoye AG, Wu AHB, Feng Y-J, Waters D. Prognostic role of troponin T versus troponin I in unstable angina pectoris for cardiac events with meta-analysis comparing published studies. Am J Cardiol 1998;81:1405-10. 6. Oltrona L, Ardissino D, Merlini PA, Spinola A, Chiodo F, Pezzano A. C-reactive protein elevation and early outcome in patients with unstable angina pectoris. Am J Cardiol 1997;80:1002-6. 7. Benamer H, Steg PG, Benessiano J, Vicaut E, Gaultier CJ, Boccara A, et al. Comparison of the prognostic value of C-reactive protein and troponin I in patients with unstable angina pectoris. Am J Cardiol 1998;82:845-50. 8. Morrow DA, Rifai N, Antman EM, Weiner DL, McCabe CH, Cannon CP, et al. C-reactive protein is a potent predictor of mortality independently of and in combination with troponin T in acute coronary syndromes: a TIMI 11A substudy. J Am Coll Cardiol 1998;31:1460-5. 9. Rebuzzi AG, Quaranta G, Liuzzo G, Caligiuri G, Lanza GA, Gallimore JR, et al. Incremental prognostic value of serum levels of troponin T and C-reactive protein on admission in patients with unstable angina pectoris. Am J Cardiol 1998;82:715-9. 10. Pietilä K, Harmoinen A, Hermens W, Simoons ML, Van de Werf F, Verstraete M. Serum C-reactive protein and infarct size in myocardial infarct patients with a closed versus an open infarct-related coronary artery after thrombolytic therapy. Eur Heart J 1993;14:915-9. 11. Tommasi S, Carluccio E, Bentivoglio M, Buccolieri M, Mariotti M, Politano M, et al. C-reactive protein as a marker for cardiac ischemic events in the year after a first, uncomplicated myocardial infarction. Am J Cardiol 1999;83:1595-9. 12. Anzai T, Yoshikawa T, Shiraki H, Asakura Y, Akaishi M, Mitamura H, et al. C-reactive protein as a predictor of infarct expansion and cardiac rupture after a first Q-wave acute myocardial infarction. Circulation 1997;96:778-84. 13. Pietilä KO, Harmoinen AP, Jokiniitty J, Pasternack AI. Serum C-reactive protein concentration in acute myocardial infarction and its relationship to mortality during 24 months of follow-up in patients under thrombolytic treatment. Eur Heart J 1996;17;1345-9.
|
|||||||||||||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |