|
Can
DPC's I. D. Blot™
Help in Assessment of H. pylori Virulence?
At the 2000 General
Meeting of the American Society for Microbiology in Los Angeles, Dr. A.
Van der Ende et al. (Academic Medical Centre, Amsterdam) presented a study
titled "Prevalence and relationship with disease of CagA-positive Helicobacter
pylori in primary care patients." The study examined the presence
of CagA-specific antibodies in different ethnicities with and without
ulcer disease. Patient CagA status was tested with DPC's I. D. Blot™
H. pylori IgG* test (serum samples), along with a CagA PCR assay (cultured
biopsy isolates). Preliminary findings suggest a utility for the I. D.
Blot assay in assessing H. pylori virulence based on the
patient antibody response.
H. pylori-associated
disease
Not everyone infected with H. pylori will develop a peptic
ulcer. It is not yet fully understood when ulcers develop, or why some
individuals develop a duodenal ulcer and others a gastric ulcer. Differences
in host, H. pylori strains, ethnicity and environmental factors
could play a role.
It is known that H.
pylori strains exhibit a significant degree of diversity. The
great variability in the H. pylori genome may explain why not all
infected individuals suffer from ulcer. Some H. pylori strains
contain particular pathogenic genes such as cytokine-associated gene A
(CagA), while others lack these genes. The CagA protein of H. pylori
has been found to be associated with more severe clinical manifestations,
such as ulcer disease and gastric cancer. Thus, discrimination between
potentially virulent strains may be relevant.
H. pylori infections
are usually diagnosed by 1) culture of gastric specimens obtained by endoscopy;
or 2) noninvasive methods such as serological testing for an antibody
response, or radiolabeled urea-based breath tests. Serological tests—mostly
immunoassays—have been widely used in epidemiological and diagnostic
evaluations. These assays are rapid, easy to perform, and can be automated.
Assay sensitivity and specificity are remarkably good.
Despite the availability
of these assays, the management of H. pylori infections is still
a matter of confusion, particularly among primary care physicians. Moreover,
numerous countries lack national guidelines for this rapidly growing area
of medicine.
Study findings
Figure 1 depicts the association between CagA-positive status and
ulcer disease in a population of primary care patients in Amsterdam. These
patients were categorized according to place of birth. Group A patients
were born in The Netherlands; group B patients were born elsewhere. Group
A exhibited a significant association between CagA-positive status and
ulcer disease: a much higher percentage of patients with ulcers were CagA
positive than were patients without ulcers. In group B patients, however,
no significant association between CagA status and ulcer disease emerged,
because nearly identical percentages of patients with and without ulcer
disease were CagA positive.
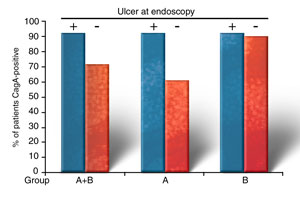
Figure
1. Association between disease and CagA-positive status in H. pylori-infected
patients.
The study also found
that the prevalence of CagA-positive H. pylori was higher among
patients born outside The Netherlands (group B) than among patients born
in The Netherlands (group A).
Figure 2 shows the
CagA-positive status by CagA PCR assay performed on culture biopsy isolates
from patients who were positive by DPC's I. D. Blot
H. pylori IgG test. The CagA PCR assay appeared to be less sensitive
than the blot assay for assessing patient CagA status. A possible explanation
is the heterogeneous distribution of a mixed population of CagA-positive
and CagA-negative H. pylori in the stomachs of the patients. A
biopsy taken from a lesion harboring a CagA-negative H. pylori
strain would yield a CagA-negative result by PCR. The use of a specific
serology immunoblot allows detection of the antibody response against
all H. pylori strains.
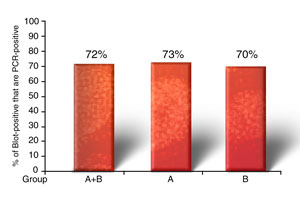
Figure
2. PCR results for 121 primary care patients with CagA-positive I. D.
Blot results.
Conclusion
This study demonstrates that the DPC I. D. Blot H. pylori IgG test
is a very useful and simple tool for identifying differences in virulence
factors between H. pylori strains. I. D. Blot can also be
used as an additional indicator of antibody response when the outcome
of an EIA is doubtful. The use of a serological test to identify specific
antibodies to CagA or other separate proteins could reduce the need for
endoscopy and could be enormously useful in decisions regarding treatment.
The study also demonstrates, however, that results may vary among different
population groups. This fact should be considered when testing in other
geographic areas.
*Sold as Analyte
Specific Reagent

|

