|
|
||||
|
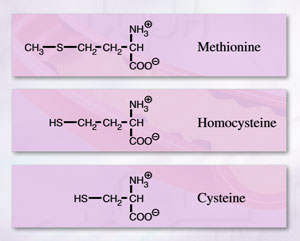
Homocysteine— Homocysteine is receiving
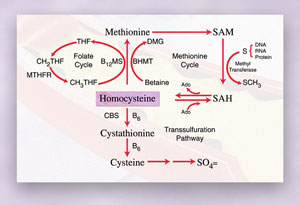
a lot of attention these days as a new risk factor What is homocysteine, where does it come from, and how is it metabolized? Homocysteine is a normal metabolite of the essential amino acid methionine (Figure 1). Structurally, it closely resembles methionine and cysteine; all three amino acids contain sulfur. They are metabolically linked to each other as shown in Figure 2. Since foods contain little or no free homocysteine, nearly all of the homocysteine in the body is derived from methionine in animal and plant proteins.
The determinants of mild hyperhomocysteinemia, commonly seen in patients with cardiovascular disease, are multifactorial and involve both genetic and acquired components. Gene-nutrient interactions such as homozygosity for thermolabile MTHFR, and low-folate nutritional status, can result in mild hyperhomocysteinemia. Approximately 12 percent of the Caucasian population is homozygous for thermolabile MTHFR. Smoking, excessive coffee consumption and lack of exercise are associated with elevations in homocysteine as well. What is hyperhomocysteinemia
and how is it determined? The term can be defined simply as "elevated
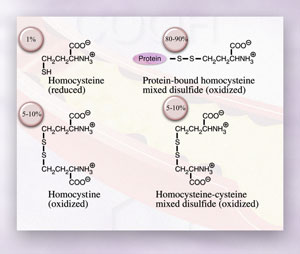
blood homocysteine" but the actual situation is more complex. When homocysteine
is transported out of cells into circulation,
Sensitive and reliable
assays for plasma total homocysteine (tHcy) were developed in the mid-
to late 1980s. This technical achievement was largely responsible for
establishing homocysteine as a major independent risk factor What is a "normal"
plasma tHcy? Until recently, the normal range for plasma tHcy was
considered to be 5 to 15 µmol/L. It is now widely accepted that the upper
limit of normal may be around 10 µmol/L for middle-aged adults and that
risk for cardiovascular disease occurs if plasma tHcy exceeds this value.
However, it is now also recognized that homocysteine levels increase with
age, perhaps as a result of micronutrient deficiencies due to malabsorption.
In the future, it is likely that age-specific reference ranges will be
established. Premenopausal women have approximately 20 percent lower values
than their male counterparts, suggesting that homocysteine metabolism
may be regulated to some extent by hormones. Patients with coronary artery
disease and other cardiovascular diseases usually have mild hyperhomocysteinemia
(>10 to 25 µmol/L) with an incidence of 30 to 50 percent. Almost all patients
with end-stage renal disease have hyperhomocysteinemia that tends to be
of an intermediate form (>25 to 50 µmol/L). Little or no homocysteine
is excreted by the normal kidney. The role of the kidney in homocysteine
metabolism and the regulation How does homocysteine injure blood vessels? Because homocysteine is a thiol, it can undergo autooxidation and oxidation with other thiols. The resulting reactive oxygen species--hydrogen peroxide and superoxide anion radical—generate oxidative stress. The concentration of plasma total cysteine is 20 to 30 times higher than that of plasma tHcy, yet cysteine, which also undergoes similar oxidative reactions, is not usually considered a risk factor. If oxidative stress is not the mechanism for homocysteine-induced vascular dysfunction, is there perhaps another, more attractive hypothesis? Yes, and it is related to direct molecular targeting by homocysteine. Recent evidence suggests that homocysteine may limit the bioavailability of nitric oxide, resulting in the impairment of flow-mediated vasodilatation. The limited bioavailability of nitric oxide could be due to nitrosothiol formation with homocysteine. Homocysteine may also target specific proteins and impair their activity and function through disulfide bond formation. The decreased binding of tissue plasminogen activator to homocysteine-modified annexin II is a case in point and may explain, in part, the procoagulant activity of homocysteine. Finally, as shown in Figure 4, homocysteine may induce the expression and secretion of chemokines such as monocyte chemoattractant protein 1 (MCP-1) and interleukin 8 (IL-8) in vascular endothelial cells. Production of these chemokines by stimulated endothelial cells would attract monocytes and neutrophils to sites of vascular injury where they could take up residence in the intimal space.
Is hyperhomocysteinemia
a treatable disease? Once a diagnosis of hyperhomocysteinemia has
been made, it is safe and easy to lower plasma tHcy in most individuals.
A cocktail of folic acid (400 to 800 µg), vitamin B12 (100 to 500 µg)
and vitamin B6 (25 to 100 mg) will reduce plasma tHcy up to Should everyone be tested for plasma tHcy? The American Heart Association has recommended that individuals with a family history of heart and cardiovascular disease be tested for plasma tHcy. Other subjects who should be tested are those with premature atherosclerosis or atherosclerosis with no known conventional risk factors such as hypertension or hyperlipidemia. Hypercoaguable profiles now routinely include plasma tHcy. Of growing concern is the increased incidence of cognitive dysfunction disorders, such as vascular dementia and Alzheimer's disease, and the possibility that micronutrient deficiencies resulting in hyperhomocysteinemia play a causative role. It may be common practice in the near future to test everyone over the age of 60 for plasma tHcy. Additional Reading
Jacobsen DW. Homocysteine and vitamins in cardiovascular disease. Clin Chem 1998;44(8 Pt 2):1833-43. Jacobsen DW. Hyperhomocysteinemia and oxidative stress: time for a reality check? Arterioscler Thromb Vasc Biol 2000;20:1182-4. Lentz SR. Mechanisms of thrombosis in hyperhomocysteinemia. Curr Opin Hematol 1998;5(5):343-9. Mansoor MA, Svardal AM, Ueland PM. Determination of the in vivo redox status of cysteine, cysteinylglycine, homocysteine, and glutathione in human plasma. Anal Biochem 1992;200(2):218-29. Refsum H, Ueland P, Nygård O, Vollset SE. Homocysteine and cardiovascular disease. Annu Rev Med 1998;49:31-62. Robinson K, Mayer EL, Miller DP, Green R, van Lente F, Gupta A, et al. Hyperhomocysteinemia and low pyridoxal phosphate. Common and independent reversible risk factors for coronary artery disease. Circulation 1995;92:2825-30. Robinson K, Gupta A, Dennis V, Arheart K, Chaudhary D, . . . Jacobsen DW. Hyperhomocysteinemia confers an independent increased risk of atherosclerosis in end-stage renal disease and is closely linked to plasma folate and pyridoxine concentrations. Circulation 1996;94:2743-8.
|
||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |