|
DPC's Third Generation PSA Assay: The Clinician's Choice for PSA Testing |
|||
| DPC’s Third Generation PSA assay gives clinicians the ability to use one PSA test for all patient applications. It has assumed an indispensable role within the realm of therapeutic PSA monitoring, prostate cancer therapy optimization and outcome prediction due to its precision at very low serum concentrations. In addition to providing accurate and timely quantification of PSA levels during and after therapy, DPC’s Third Generation PSA assay is also well suited for general prostate cancer screening purposes. Prostate
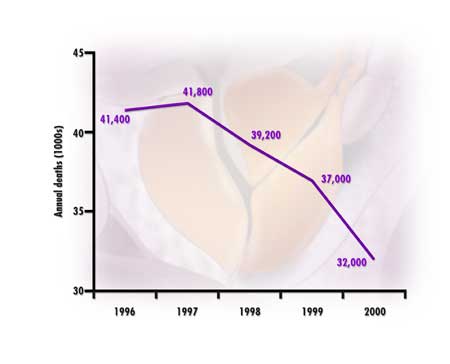
cancer screening controversy Other technologies may also be contributing to earlier detection of prostate cancer. These include the availability of free PSA and use of the free-to-total PSA ratio; improved ultrasonography and prostate biopsy methods; and the wider application of risk assessment algorithms involving, for example, age-adjusted PSA, prostate gland volume, transition zone volume and PSA density. The decline in prostate cancer mortality may also be explained, in part, by improved treatments for early-stage disease and better follow-up care, as reviewed below. Current PSA studies indicate that cancer cases exhibit a slow linear PSA phase initially, followed by a rapid exponential phase, and that PSA levels begin to increase exponentially approximately 7 to 9 years before diagnosis.9 Experts agree on the benefits of calculating PSA doubling times (PSADT), which are derived from a baseline measurement and subsequent PSA values obtained at appropriate intervals. Published data indicate that the median PSADT for localized prostate cancer is 4 years, but it is shorter in higher clinical stages and worse histologic grades.10,11 In contrast, PSADT in age-matched controls is much longer.12 Because the IMMULITE® and IMMULITE® 2000 Third Generation PSA assays possess outstanding low-end precision, they are ideal tools for following PSA trends over time and obtaining accurate PSADT calculations.
Monitoring
treatment
Studies
using DPC’s Third Generation PSA assays have established the value of
highly sensitive PSA assays to detect early prostate cancer relapse following
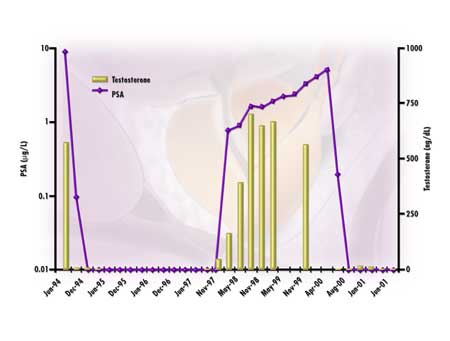
radical prostatectomy.13-15 Witherspoon et al. demonstrated
an average 18-month lead time in detecting disease progression using DPC’s
IMMULITE Third Generation PSA compared to a conventional PSA assay (Figure
2).13 Vassilikos et al. confirmed this lead time and was able,
over a 4-year follow-up period, to define a group of patients having rapid
PSA relapse.14 Doherty et al. showed that a single baseline
PSA level < 0.01 µg/L measured 4 to 6 weeks postsurgery indicates a lower
probability of disease progression.15 On multivariate analysis,
failing to achieve a PSA nadir of
Definitive radiation therapy in which the gland remains in situ rarely results in an undetectable PSA, even when cure is achieved.19 However, there is a general consensus that PSA levels reaching a nadir < 1.0 µg/L are associated with improved biochemical disease-free survival.16,17 Disease progression is strongly suspected if the PSA rises on consecutive determinations. The use of a highly sensitive PSA assay, such as the IMMULITE or IMMULITE 2000 Third Generation PSA, can help detect early disease progression in radiation-treated patients. For patients suffering PSA progression following primary surgery, viable treatment options include salvage radiation or androgen deprivation therapy (ADT). Salvage radiation treatment will benefit only those patients with proven residual cancer in the prostatic fossa, whereas ADT can benefit those with residual cancer and/or metastatic disease. Serial PSA measurements in the months following surgery can be used to determine whether a patient is more or less likely to benefit from salvage radiation therapy.18-20 Undetectable baseline PSA levels defined (by conventional assays) as < 0.2 µg/L following surgery, which later become detectable and progressively rise, suggest locally recurring cancer in the prostatic fossa.18 (See Figure 2 for an example.) On the other hand, detectable PSA levels at baseline which show progressive increases may represent microscopic metastatic disease that was present prior to radical prostatectomy. In the former scenario, salvage radiation treatment may be indicated, whereas systemic salvage treatment using ADT would appear to be indicated in the latter. Early PSA relapse, unfavorable Gleason sum and rapid PSADT are also associated with prostate cancer metastases following both surgery and radiation treatment.26,27 The lead time afforded by ultrasensitive PSA assays and their superior low-end precision identifies patients with early disease relapse and can help guide medical decision-making regarding salvage therapy options.
For primary or salvage ADT, PSA is the most sensitive surrogate marker of disease activity with which to judge treatment efficacy. Even in advanced metastatic disease, achieving an undetectable PSA < 0.2 or < 0.3 µg/L within 6 months of starting ADT, distinguishes patients with a favorable and persisting response to ADT from those in whom only a limited response can be expected.21,28 For patients with less extensive disease, response to ADT is likely to be extremely favorable.22 Attainment and maintenance of a PSA < 0.05 µg/L for a year or more while on ADT can be used to identify patients with androgen-dependent prostate cancer, in whom intermittent ADT is feasible.23-25 Patients with low-volume disease, such as those having PSA relapse, can often enjoy prolonged time-off treatment with improved quality of life.25 When retreatment is indicated in such patients, due to a rising PSA or other clinical findings, an excellent response to ADT can be anticipated. Conclusion Table 1. Relevant PSA values in various treatment modalities.
References 2. American Foundation for Urologic Disease. Prostate cancer resource guide. Baltimore, MD: The Foundation, 1999. . 3. US Preventative Services Task Force. Guide to clinical preventive services. 2nd ed. Washington, DC: US Dept. of HHS, PHS, Science, Office of Disease Prevention and Health Promotion, Inc., 1996. 4. American Cancer Society: Prostate cancer and cancer detection guidelines, 1999. Atlanta, GA: The Society, 1999. 5. Centers for Disease Control and Prevention. Screening with the prostate-specific antigen test-Texas 1997. Morbid Mortal Weekly Rep 2000 Sept 15;49(36). 6. Stanford JL, Feng Z, Hamilton AS, Gilliland FD, Stephenson RA, Eley JW, Albertsen PC, Harlan LC, Potosky AL. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA 2000 Jan 19;283(3):354-60. 7. Potosky AL, Miller BA, Albertsen PC, Kramer BS. The role of increasing detection in the rising incidence of prostate cancer. JAMA 1995 Feb 15;273(7):548-52. 8. American Cancer Society. Mortality Statistics, 1995-2000. From the Web site of the American Cancer Society: http://www.cancer.org 9. Crawford ED, DeAntoni EP, Ross CA. The role of prostate-specific antigen in the chemoprevention of prostate cancer. J Cell Biochem Suppl 1996;25:149-55. 10. el-Galley RE, Petros JA, Sanders WH, Keane TE, Galloway NT, Cooner WH, et al. Normal range prostate-specific antigen versus age-specific prostate-specific antigen in screening prostate adenocarcinoma. Urology 1995 Aug;46(2):200-4. 11. Schmid HP. Tumour markers in patients on deferred treatment: prostate specific antigen doubling times. Cancer Surv 1995;23:157-67. 12. Carter HB, Pearson JD, Metter EJ. Longitudinal evaluation of prostate-specific antigen levels in men with and without prostate disease. JAMA 1992;267(16):2215-20. 13. Witherspoon LR, Lapeyrolerie T. Sensitive prostate specific antigen measurements identify men with long disease-free intervals and differentiate aggressive from indolent cancer recurrences within 2 years after radical prostatectomy. J Urol 1997 Apr;157(4):1322-8. 14. Vassilikos EJ, Yu H, Trachtenberg J, Nam RK, Narod SA, Bromberg IL, Diamandis EP. Relapse and cure rates of prostate cancer patients after radical prostatectomy and 5 years of follow-up. Clin Biochem 2000 Mar;33(2):115-23. 15. Doherty AP, Bower M, Smith GL, Miano R, Mannion EM, Mitchell H, et al. Undetectable ultrasensitive PSA after radical prostatectomy for prostate cancer predicts relapse-free survival. Br J Cancer 2000 Dec;83(11):1432-6. 16. Lee WR, Hanlon AL, Hanks GE. Prostate specific antigen nadir following external beam radiation therapy for clinically localized prostate cancer: the relationship between nadir level and disease-free survival. J Urol 1996 Aug;156(2 Pt 1):450-3. 17. Aref I, Eapen L, Agboola O, Cross P. The relationship between biochemical failure and time to nadir in patients treated with external beam therapy for T1-T3 prostate carcinoma. Radiother Oncol 1998 Aug;48(2):203-7. 18. Cadeddu JA, Partin AW, DeWeese TL, Walsh PC. Long-term results of radiation therapy for prostate cancer recurrence following radical prostatectomy. J Urol 1998 Jan;159(1):173-7; discussion 177-8. 19. Forman JD, Meetze K, Pontes E, Wood DP Jr, Shamsa F, Rana T, et al. Therapeutic irradiation for patients with an elevated post-prostatectomy prostate specific antigen level. J Urol 1997 Oct;158(4):1436-9; discussion 1439-40. 20. Egawa S, Matsumoto K, Suyama K, Soh S, Kuwao S, Iwamura M. Limited suppression of prostate-specific antigen after salvage radiotherapy for its isolated elevation after radical prostatectomy. Urology 1999 Jan;53(1):148-54. 21. Zagars GK, Sands ME, Pollack A, von Eschenbach AC. Early androgen ablation for stage D1 (N1 to N3, M0) prostate cancer: prognostic variables and outcome. J Urol 1994 May;151(5):1330-3. 22. Fowler JE Jr, Pandey P, Seaver LE, Feliz TP, Braswell NT. Prostate specific antigen regression and progression after androgen deprivation for localized and metastatic prostate cancer. J Urol 1995 Jun;153(6):1860-5. 23. Higano CS, Ellis W, Russell K, Lange PH. Intermittent androgen suppression with leuprolide and flutamide for prostate cancer: a pilot study. Urology 1996 Nov;48(5):800-4. 24. Grossfeld GD, Small EJ, Carroll PR. Intermittent androgen deprivation for clinically localized prostate cancer: initial experience. Urology 1998 Jan;51(1):137-44. 25. Strum SB, Scholz MC, McDermed JE. Intermittent androgen deprivation in prostate cancer patients: factors predictive of prolonged time off therapy. Oncologist 2000;5(1):45-52. 26. Fowler JE Jr, Pandey P, Braswell NT, Seaver L. Prostate specific antigen progression rates after radical prostatectomy or radiation therapy for localized prostate cancer. Surgery 1994 Aug;116(2):302-5; discussion 305-6. 27. Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999 May 5;281(17):1591-7. 28. Stamey TA, Kabalin JN, Ferrari M, Yang N. Prostate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. IV. Anti-androgen treated patients. J Urol 1989 May;141(5):1088-90.
|
||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |