|
IgG Avidity Testing: Distinguishing Primary from Latent Toxoplasma Infection |
|||
|
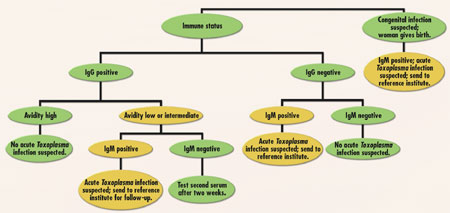
When the host is exposed to the antigen a second time, a markedly different kinetic pattern is observed. The period between exposure and the appearance of detectable antibody is much shorter. Whereas IgM is initially predominant in the primary response, IgG levels exceed those of IgM overwhelmingly throughout the entire secondary immune response. The IgG also shows a much more rapid rise in titer, a longer plateau, and a slower decline than it does during the primary immune response. In some cases, the IgM response is seen only in the primary immune response, while in others, IgM antibodies may be seen in a secondary response that resembles the primary immune response. Nonetheless, the IgM titer is dwarfed by the high IgG titer. Such characteristics are important to consider when basing clinical diagnosis on infectious disease serology. Using an avidity assay in conjunction with IgG and IgM antibody response provides a much clearer indicator of acute infection. The problem with relying on only IgG and IgM antibody response is that IgM can persist for months after primary infection and, as already mentioned, can reappear during recurrent infections. In addition, IgG antibodies formed in the secondary antibody response are of higher avidity (binding strength) than those of the primary response. Initially, the antibodies formed are mostly of relatively low avidity. Over time, however, the antibodies with high avidity for the antigen increase, while those with low avidity decrease in titer. Can the clinical laboratory exploit this phenomenon as an aid in diagnosis? In the late 1980s, Hedman et al.1 introduced a new method of detecting recently acquired Toxoplasma infection, based on the strength of the binding of specific IgG to multivalent Toxoplasma antigen. Toxoplasma gondii can cause serious damage to the fetus when a pregnant woman acquires a primary infection. The presence of Toxoplasma-specific IgM in serum as an indicator of recent infection is unreliable, due to differences in the persistence of these antibodies. In some patients, specific IgM may persist for months or even years following a primary infection. Jenum et al.2 observed that women with a possible acute infection have a low mean IgG avidity, based on a combination of positive specific IgM and a high Sabin-Felman dye titer of greater than 300 IU/mL (the gold standard test). In women positive for Toxoplasma-specific IgM, but with a low titer, the mean IgG avidity was high. In a third group of women with latent infection without detectable Toxoplasma-specific IgM, the mean IgG avidity was high also. The introduction of Toxoplasma-specific IgG avidity testing on IgM-positive samples collected in the first trimester of pregnancy can eliminate false-positive results that would suggest recent infection. Thus, IgG avidity testing can prevent unnecessary anxiety, as well as additional examinations and treatment. In my opinion, one can use this avidity assay in two ways: to improve the diagnostic routine and to discriminate between primary and latent infection. If IgG and IgM results are positive, one can perform an avidity assay and, in the case of high avidity, rule out recent infection. A finding of low avidity indicates the need for further testing by a reference laboratory. Furthermore, all IgG-positive results should be followed by an avidity assay. A high-avidity result rules out a recent infection, while a low-avidity result should be followed by an IgM assay. In the case of a positive IgM result, a recent infection is almost certain. A second sample should be requested to establish a baseline, or the serum sample should be sent to a reference laboratory for confirmation of results. (See Figure 1.) Clinical laboratory diagnostics can now discriminate between primary and latent infection more accurately by examining the different binding capacities of IgG molecules.
|
||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |