  |
Editor’s note: This article was originally published in Dutch in DIAGNED,
the quarterly magazine of the Dutch Association of Diagnostics Manufacturers.
DPC Nederland, a member of the Association, arranged for the writing and
publication of the article, and provided the English translation below,
with permission of DIAGNED.
Symptoms
and prevalence
Systemic lupus erythematosus (SLE, LE), also known as lupus, is a rare,
rheumatic autoimmune disease in which the patient produces antibodies
that are directed against his own tissue. These autoantibodies can cause
inflammation in any organ or area of the body, including skin, joints,
kidneys, brain, heart and lungs. The disease comes and goes. The course
and intensity is unpredictable and is not the same from one patient to
another. Environmental factors such as infections, certain antibiotics
and other drugs, ultraviolet light, extreme stress, and hormones (particularly
estrogen) are known to play a key role in triggering the disease. A genetic
predisposition also appears to be involved.
SLE
occurs mainly in young people, aged between 20 and 40, and is nine to
fifteen times more common in women than in men. People of African, American
Indian, and Asian origin appear to have a higher incidence than Caucasians.
Dr.
Hendrika Bootsma, rheumatologist at the university hospital in Groningen,
The Netherlands, has been working on the disease for about ten years.
SLE prevalence in that country is approximately 40 in 100,000. Patients
come with a very wide range of complaints and may therefore see various
specialists before they are referred to the rheumatology department. Dr.
Bootsma reports chronic tiredness as the most frequent complaint. In addition,
before the disease flares up, SLE patients often display flu-like symptoms,
skin disorders and joint complaints. The general nature and variety of
clinical symptoms makes diagnosis difficult. Sometimes patients suffer
from complaints for years before finally receiving a diagnosis of SLE.
Dr. Bootsma uses the eleven international criteria for diagnosis (Table
1); the identification of four of them leads to a diagnosis of SLE.
Table
1. Criteria for the diagnosis of lupus.2
| Criterion |
Comments |
| Malar
rash |
Rash
over the cheeks. |
| Discoid
rash |
Red
raised patches. |
| Photosensitivity |
Reaction
to sunlight: development or exacerbation of skin rash. |
| Oral
ulcers |
Ulcers
in the nose or mouth, usually painless. |
| Arthritis |
Nonerosive
arthritis in two or more peripheral joints. |
| Serositis |
Pleuritis
or pericarditis. |
| Renal
disorder |
Excessive
protein in the urine (>0.5 g/day or 3+ on test sticks) and/or cellular
casts derived from red, white or renal tubular cells. |
| Neurologic
disorder |
Seizures
and/or psychosis in the absence of drugs or other metabolic disturbances
know to cause such symptoms |
| Hematoligic
disorder |
Hemolytic
anemia or leukopenia (WBC count < 4,000 cells/mm3) or lymphopenia
(lymphocytes < 1,500/mm3) or thrombocytopenia (platelets < 100,000/mm3).
Leukopenia or lymphocytopenia must be detected on at least two occasions.
Thrombocytopenia must be detected in the absence of drugs that can
induce it. |
| Anti-nuclear
antibody |
Positive
test for anti-nuclear antibodies (ANA) in the absence of drugs that
can induce it. |
| Immunologic
disorder |
Positive
anti-double-stranded DNA test, positive anti-Sm test, positive anti-phospholipid
antibody such as anticardiolipin, or false-positive syphilis test
(VDRL). |
Diagnosis
Although the diagnosis is established on clinical grounds, it is strongly
supported by laboratory testing. The relevant laboratory tests seek to
establish the presence of autoantibodies. Specificity and sensitivity
are essential, but no single test offers 100 percent performance for either
criterion. Dr. Bootsma usually uses a combination of two tests. The first
is anti-nuclear antibody (ANA) testing in patient blood, to detect antibodies
directed against elements of the cell nuclei. It is a simple and extremely
sensitive test which is positive in over 95 percent of SLE patients. Lack
of specificity for SLE—the
test gives positive results for other autoimmune diseases such as rheumatoid
arthritis or Sjögren’s syndrome—requires
the use of a second test in the event of a positive ANA result. The anti-double-stranded
DNA test (anti-DNA for short) is more specific for SLE and can provide
a quantitative result.
Preventing
disease flare-ups
If the patient remains under expert supervision, the prognosis in terms
of life expectancy and quality of life is far more favorable than it was
a few decades ago. The most worrisome times are the exacerbation or so-called
flare-up periods, during which the disease strikes with its full intensity
and serious functional disorders can occur in affected organs. One of
the most serious manifestations, observed in 50 to 70 percent of patients,
is nephritis. Although in many cases the organs recover again, permanent
damage can also occur. Avoiding flare-ups means less patient distress
and less chance of permanent, serious organ damage.
Desiring
to improve her patients’ quality of life, Dr. Bootsma sought to predict
flare-ups and offer preventive treatment. She and her colleagures found
that the anti-DNA concentration appears to be a suitable indicator of
an impending exacerbation. Conducting their research at the university
hospitals in Groningen and Utrecht, they measured the blood anti-DNA concentration
in 156 patients monthly. In 46 patients they found a significant increase
at a certain moment. The striking thing was that at that time, these patients
had no complaints at all, nor did they show any clinical symptoms. Twenty-four
of the 46 patients received conventional treatment and 22 received preventive
treatment with 30 mg of the anti-inflammatory prednisone. Of the 24 patients
on conventional treatment, 20 of them suffered a flare-up; whereas of
the 22 patients treated with prednisone, only two suffered a flare-up.
(See Figure 1.) Dr.
Bootsma and her colleagues have published papers and addressed international
congresses on their findings. The university hospital in Groningen has
implemented an extensive monitoring system to follow anti-DNA concentrations
in the blood of SLE patients.
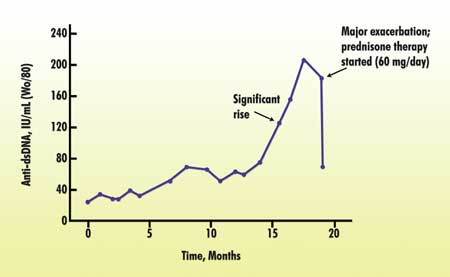
Figure
1. Effect of prednisone treatment on anti-DNA levels in SLE. A rising
anti-DNA concentration in the blood often indicates an imminent flare-up
of the disease. Treatment with the anti-inflammatory prednisone reduces
anti-DNA antibody levels and is almost certain to prevent a flare-up.1
Dr.
Bootsma admits that this approach requires intense supervision and careful
organization. The patient must be motivated enough to have a blood sample
taken every month, and the laboratory must keep careful records. In addition,
the doctor in attendance must be disciplined and follow the measurements
up closely. Whenever Dr. Bootsma observes a significant increase, she
alerts the patient to prepare for treatment, even in the absence of significant
complaints.
A
need for more research
Despite
progress, a great deal of further research is required. It is desirable,
for example, to find alternatives to drugs with unpleasant side effects.
The causes and triggers of the disease remain to be fully elucidated.
Although it is difficult to obtain funding for research into a rare disease
such as SLE, Dr. Bootsma believes the rewards would far outweigh the costs.
“Few people seem to realize the potential added return on SLE research.
After all, this is research into the immune system and there are more
and more indications that deficiencies in immune system function are also
closely involved in the development of tumors.” Possible cost savings
are also often overlooked. “Although an anti-DNA test and prednisone treatment
are not cheap, these costs are still amply offset by the costs of admittance
to hospital, treatment of possibly damaged organs, and the diminished
quality of life.”
References
1.
Spronk PE, Bootsma H, Kallenberg CG. Anti-DNA antibodies as early predictor
for disease exacerbations in SLE. Guideline for treatment? Clin Rev Allergy
Immunol 1998 Fall;16(3):211-8.
2. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al.
The 1982 revised criteria for the classification of systemic lupus erythematosus.
Arthritis Rheum 1982 Nov;25(11):1271-7.
|

