|
||||||
|
New!
Vitamin B12 and Folic Acid Assays on IMMULITE®
2000
Clinical
significance Pernicious anemia is the result of vitamin B12 deficiency due to a lack of available intrinsic factor (IF), a gut glycoprotein necessary for B12 absorption. This anemia appears most frequently in older populations; as many as 800,000 elderly people in the United States may be undiagnosed and untreated.2 2. Carmel R. Prevalence of undiagnosed pernicious anemia in the elderly. Arch Intern Med 1996;157:1097-100. Elevated vitamin B12 levels are rare but can occur in chronic renal failure and in certain leukemias and liver conditions.3 3. Tietz NW (editor). Clinical guide to laboratory tests. 3rd ed. Philadelphia: Saunders, 1995; 637. Folic acid deficiency is the most common vitamin deficiency and manifests in many of the malnutrition and malabsorption syndromes associated with vitamin B12 deficiency.4 4. Tietz NW (editor). Clinical guide to laboratory tests. 3rd ed. Philadelphia: Saunders, 1995; 246-7. Prevalence is highest in alcoholics with liver disease, the elderly, and pregnant women. Adequate folic acid levels are necessary in early pregnancy to prevent spina bifida and anencephaly.5 5. Folic acid: powerful tool against birth defects. Food Insight 1995 Jul/Aug. A variety of drugs may contribute to folate deficiencies; these include methotrexate; anticonvulsants such as phenobarbital, phenytoin and valproic acid; oral contraceptives; alcohol; antacids and bicarbonate.6 6. Tietz NW (editor). Clinical guide to laboratory tests. 3rd ed. Philadelphia: Saunders, 1995; 246. Moghadasian MH, et al. Homocysteine and coronary artery disease. Arch Int Med 1997;157:2299-308. Fallest-Strobl PC, et al. Homocysteine: a new risk factor for atherosclerosis. Am Fam Physician 1997;56:1607-12. High folic acid levels may occur in patients with B12 deficiency, pernicious anemia and vegetarian diets. Folate toxicity is extremely rare.7 7. Tietz NW (editor). Clinical guide to laboratory tests. 3rd ed. Philadelphia: Saunders, 1995; 247. An inverse relationship exists between vitamin B12 and folate levels and levels of the amino acid homocysteine. 88. Langman LJ, Cole DEC. Homocysteine. Crit Rev Clin Lab Sci 1999;36:365-406.,13 13. Selhub J, Jacques PF, Wilson PW, Rush D, Rosenberg IH. Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA 1993;270:2693-8. Elevated homocysteine has been implicated in heart disease, stroke and other diseases of the blood vessels.8 8. Langman LJ, Cole DEC. Homocysteine. Crit Rev Clin Lab Sci 1999;36:365-406.
In the vitamin B12 assay, serum or plasma samples are chemically pretreated in an automated cycle to release vitamin B12 from binding proteins. An aliquot of pretreated sample, hog intrinsic factor (HIF) and an alkaline phosphatase-labeled monoclonal antibody against HIF (anti-HIF MAb) are introduced into the reaction tube containing a vitamin B12-coated bead. Patient B12 and B12 on the bead compete for HIF. A fraction of the enzyme-labeled anti-HIF MAb becomes complexed with the HIF that binds to the vitamin B12 on the bead. The chemiluminescent substrate is added and undergoes hydrolysis in the presence of the enzyme label. This reaction yields a result that relates inversely to the vitamin B12 concentration in the patient sample. The anti-HIF MAb used in this assay was specifically produced and selected to bind HIF without interfering with the latter’s ability to bind vitamin B12. In the folic acid assay, serum, plasma or whole blood hemolysate samples are chemically pretreated in two automated cycles to release folate. (Whole blood hemolysates require an off-line dilution with ascorbic acid solution.) An aliquot of pretreated sample, ligand-labeled folate and folate binding protein (FBP) are added to the reaction tube containing a bead coated with a monoclonal antibody against folate binding protein (anti-FBP MAb). Folate from the patient sample competes with the ligand-labeled folate for the FBP, and ligand-labeled folate–FPB complex binds to the anti-FBP antibody on the bead. Alkaline phosphatase-labeled anti-ligand is added and binds to the ligand-labeled folate in the complex immobilized on the bead. Substrate addition initiates the chemiluminescent reaction, yielding a result that relates inversely to the folate concentration in the patient sample. In both assays, unbound materials are removed by a patented centrifugal wash technique. The chemiluminescent substrate, a phosphate ester of adamantyl dioxetane, yields an unstable intermediate in the presence of the alkaline phosphatase label. The continuous production of this intermediate results in a sustained emission of photons, allowing multiple readings for enhanced precision. When displaying results, the IMMULITE 2000 automatically adjusts for dilution. Convenient, reliable
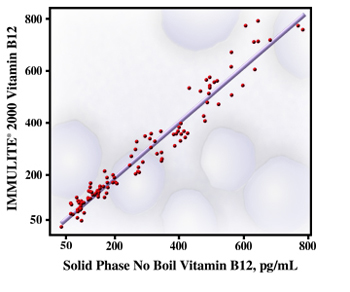
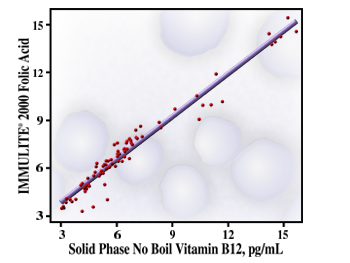
anemia testing Automating the sample pretreatment is not only convenient; it also allows for uniform sample handling for enhanced precision. In addition, the assays were designed to provide reliable results and overcome the difficulties encountered by some manufacturers’ tests when assaying certain sample types such as those from renal dialysis patients.9 9. Roberts WL, Schwartz EL, Moulton L. Performance characteristics of the IMMULITE 2000 serum folic acid assay [abstract]. Clin Chem 2000;46(6 Suppl):A110-1. IMMULITE 2000 Vitamin B12 and Folic Acid compare well with DPC’s Solid Phase No Boil assays—long-time industry standards. (The figures display correlation data.) Calibration ranges are wide enough to accommodate reference values and those found in a broad array of clinical conditions. For patients receiving supplemental therapy, particularly those receiving folate whose results may exceed the reportable range, the system is capable of automatic sample dilutions. Precision for Vitamin B12, expressed in terms of CVs, ranges from 5 to 14% over the calibration range; that for Folic Acid is excellent, ranging from 5 to 9%. Linearity is good for both assays. Whereas some manufacturers’ folic acid assays lose linearity with increasing concentrations,10 10. Billen J, Zaman Z, Claeys G, Blanckaert N. Limited dynamic range of a new assay for serum folate [letter]. Clin Chem 1999;45:581-2. Manzella S, Gronowski A, Ladenson J, Scott MG. Limited linear range of the Abbott AxSYM serum and erythrocyte folate methods [letter]. Clin Chem 1999;45:582-3. the IMMULITE 2000 assay demonstrates uniform linearity across its calibration range, for reliable results at the high end of the calibration range. The system advantage
The introduction of the two new assays for anemia consolidates this important testing category on the IMMULITE 2000 system. The IMMULITE 2000 also offers a broad menu of routine and esoteric assays related to reproductive endocrinology, thyroid function, diabetes, bone integrity, cancer and more, accommodating a wide range of the laboratory’s test requirements. The system provides convenient random access, ease of use, and reliable system performance, all backed by superior technical and customer service.
Conclusion
|
||||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |


 Assays
for vitamin B12 and folic acid aid in the clinical diagnosis and treatment
of anemia. High-volume labs can now perform vitamin B12 and folic acid
testing on DPC’s IMMULITE®
2000 random access, chemiluminescent immunoassay system. IMMULITE 2000
Vitamin B12 and Folic Acid assays offer the convenience of fully automated,
on-board sample pretreatment, and quality performance equivalent to that
of DPC’s time-tested, isotopic Solid Phase No Boil method. These important
menu additions allow the laboratory’s anemia testing workload to be handled
in the same manner as other immunoassay testing that the laboratory currently
performs on the IMMULITE 2000 system.
Assays
for vitamin B12 and folic acid aid in the clinical diagnosis and treatment
of anemia. High-volume labs can now perform vitamin B12 and folic acid
testing on DPC’s IMMULITE®
2000 random access, chemiluminescent immunoassay system. IMMULITE 2000
Vitamin B12 and Folic Acid assays offer the convenience of fully automated,
on-board sample pretreatment, and quality performance equivalent to that
of DPC’s time-tested, isotopic Solid Phase No Boil method. These important
menu additions allow the laboratory’s anemia testing workload to be handled
in the same manner as other immunoassay testing that the laboratory currently
performs on the IMMULITE 2000 system.