| |
DPC
produces an array of kits used to aid in the diagnosis of a variety of
infectious diseases. Most of these assays do not determine the presence
of the causative agent directly, but instead indicate an immune response
by detecting the host's production of IgG or IgM antibodies. Monitoring
IgG, however, is not always an indication of acute disease: many infectious
pathogens persist in latency after the primary infection has resolved,
resulting in continuing IgG production. Acute illness is often better
characterized by assaying for antigen-specific IgM antibodies, which are
produced early in the infection—usually peaking as IgG levels begin
to rise, then declining to very low or undetectable levels within a few
months.
Indirect
sandwich assay vs. µ-capture assay
DPC's Research and Development team knows that flexibility and ingenuity
are the essential mainstays of a successful assay-engineering program.
In many cases, what works admirably for the detection of one analyte returns
only fair results for another, especially in the case of infectious disease,
where crossreactivity between antigens and antibodies can severely limit
the diagnostic utility of a test. Accordingly, DPC employs different methods
for determining the presence of specific IgM as an indicator of acute
infection. Two of these methods, the indirect sandwich assay and the µ-capture
assay, are highlighted and reviewed in DPC's new technical report, Infectious
Disease Diagnosis: Different Assay Formats for the Serological Detection
of Antigen-Specific IgM. Besides supplying an overview of the immunology
underlying these protocols, the report outlines the interfering factors
inherent in each format and how assay design assures the best specificity
and sensitivity achievable. Brief discussions of DPC's CMV and toxoplasma
IgM assays are presented as practical examples of the two methodologies.
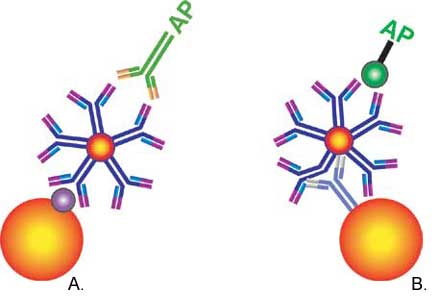
The
soon-to-be-released CMV IgM assay utilizes indirect solid-phase ELISA
to generate a qualitative result. In this kit, CMV antigen immobilized
on a bead is used to capture CMV IgM from either serum or plasma. An enzyme-labeled
secondary IgG antibody directed against IgM is then added and a signal
proportional to the antibody concentration is generated upon addition
of the chemiluminescent substrate (Figure 1A).
In
the µ-capture IgM protocol employed by DPC's new toxoplasma screen, IgM
from either serum or plasma is captured not by an antigen, but by an anti-human
IgM antibody immobilized on the bead. Anti-human IgM is directed against
the conserved region of the µ heavy chain (hence the assay name), which
contains amino acid sequences unique to IgM. Bound antigen-specific IgM
is then detected by the addition of alkaline phosphatase-labeled Toxoplasma
gondii membrane antigen in the presence of the chemiluminescent substrate
(Figure 1B).

|
|
Figure 1. Indirect
vs. µ-capture formats: A, indirect sandwich format; and B, µ-capture
format.
|
Interfering
factors
Different factors present in the serum of both healthy and sick individuals
can interfere with the correct binding of IgM in both types of assays,
yielding either false-positive or false-negative results. Sources
of interference include heterophilic antibodies, crossreactions with
evolutionarily similar antigens, antigen-specific IgG and rheumatoid
factor (RF) (Figure 2). If serum contains heterophilic antibodies,
which are often present in patients who have been regularly exposed
to animals or animal sera, they can link to both bound IgG and the
signal antibody, creating a false-positive result (Figure 2B). Crosslinkage
and false positives can also result if the patient has been simultaneously
infected with an evolutionarily related virus or other pathogen and
is producing abundant IgM (Figure 2C) or IgG. Antigen-specific IgG
may be present in individuals who have already begun to seroconvert
from IgM even though the patient may still be in the acute phase of
infection, or as the result of a previous infection. In the indirect
method, high levels of antigen-specific IgG compete with and inhibit
the binding of antigen-specific IgM to the capture antigen, yielding
a false negative (Figure 2D). If RF is present, it can bind to the
competing bound antigen-specific IgG as well as the labeled IgG, yielding
a false positive (Figure 2E). (RF is found in patients with rheumatoid
arthritis but may also be found in the presence of a number of other
illnesses, including viral infection, and even in healthy individuals.)
In most cases, addition of a wash step using anti-human IgG (Fc portion)
removes these contaminants from sandwich assays. |
| |
|
|
|
Figure
2. Proper binding (A) and various modes of interference (B-E) in
the measurement of IgM.
|
| |
|
|
Learning
more about these assay designs
Greater detail on the mechanisms and functionality of these assays is
presented in DPC's new technical report, Infectious Disease Diagnosis:
Different Assay Formats for the Serological Detection of Antigen-Specific
IgM, which is now available on the DPC website (www.dpcweb.com)
or from your local DPC representative (catalog number ZB232).
|