| |
Traditionally,
allergy specialists were considered to have the primary responsibility
for the diagnosis and care of allergic patients. Because of recent changes
in the healthcare systems in many parts of the developed world, however,
the primary care physician is now expected to make an allergy diagnosis
and decide whether to treat or refer the patient to a specialist. DPC
offers 3gAllergy™, an ultrasensitive, third-generation assay for the quantitative,
in vitro measurement of allergen-specific IgE. 3gAllergy is a reliable,
convenient tool that can help the primary care physician diagnose and
monitor patients with allergic disease or qualify and refer complex cases
to an allergy specialist, thereby improving patient care.
Changing
diagnostic methods
The preferred diagnostic tool of allergy specialists has long been in
vivo testing, typically the skin prick test. This test is a safe and sensitive
procedure in the hands of a trained and skilled specialist, whose knowledge
is necessary for correct interpretation. In addition, the risk of an anaphylactic
reaction to the procedure requires a trained staff and a properly equipped
office.
In
vitro allergen-specific IgE testing began with the first-generation radioallergosorbent
test (RAST), introduced in the early 1970s. It found limited acceptance
among allergists and laboratories worldwide because it failed to correlate
closely with the skin prick test in terms of sensitivity, specificity
and reproducibility, nor did it offer the automation and system productivity
that laboratories desired. The second-generation RAST, introduced in the
1980s, exhibited good correlation to skin prick testing in terms of specificity,
positive predictive value (PPV) and negative predictive value (NPV),1,2
and it offered an improved turnaround time. But it was still less sensitive
than the skin prick test and still fell short of addressing laboratories'
need for automation and random access. The same decade saw the advent
of managed care and a broadening of the responsibility placed on the primary
care physician.
Among
non-allergy specialists, it is a common practice today to bypass diagnostic
testing and to jump from symptoms to prescription of treatment on the
assumption of allergy. But as many as two-thirds of patients with allergy-like
symptoms may be misdiagnosed as allergy patients, according to a US study
conducted in a managed care organization, and over 65 percent of patients
who took antihistamines did not need them because they did not have allergy.3

|
|
|
Click
image to enlarge.
|
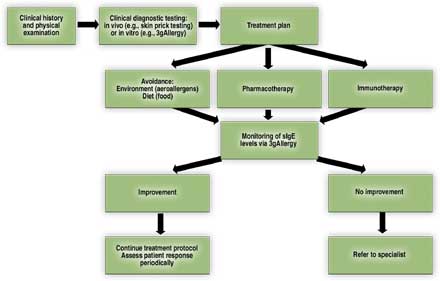
| Figure 1. A complete
testing paradigm such as the one pictured here includes clinical diagnostic
testing-either in vivo or in vitro. In vitro testing with an assay
such as DPC's 3gAllergy allows for the identification of allergen-specific
IgE (sIgE) and monitoring of the the treatment plan's effect on circulating
sIgE levels. |
A simpler solution for physicians and laboratories
In 2001, DPC introduced on its IMMULITE® 2000 immunoassay system the first
FDA-cleared, third-generation assay for allergen-specific IgE. Named 3gAllergy
and now offering more than 360 allergens and allergen panels, it is a
convenient tool to assist the primary care physician in arriving at a
diagnosis of allergy when used in combination with a clinical examination
and patient history. 3gAllergy is a safe alternative to in vivo methods
and therefore particularly desirable for use with patients who have a
history of anaphylactic reactions. It is well suited for patients with
skin conditions such as eczema or dermatographism, and it allows testing
of patients without requiring them to stop taking their allergy medications.
Numerous studies demonstrate good correlation with in vivo and laboratory
methods.4
3gAllergy
also addresses the needs of the laboratory. Now available on both the
IMMULITE 2000 and the IMMULITE® 2500, it provides full automation, random
access processing, a rapid turnaround time of about one hour, and consolidation
of allergy testing and other immunoassays on the same platform. Because
3gAllergy is performed just like any other immunoassay, it eliminates
the need for dedicated equipment or extensive training of staff.
The
lowest detection limit of any specific IgE assay
3gAllergy has advanced allergy testing to a new level of precision, analytical
sensitivity and functional sensitivity. Its enzyme-enhanced chemiluminescence
technology detects IgE at a lower concentration than any other in vitro
allergy immunoassay, for a functional sensitivity of 0.2 kU/L and a low-end
detection limit of 0.1 kU/L. 3gAllergy also demonstrates linearity under
dilution down to this detection limit, with dilution factors ranging from
1 to 1000 rather than from 1 to 100 as with second-generation in vitro
IgE tests.5 What this means for patient care is that it is
possible to detect allergy earlier and start treatment sooner.
Importance
of diagnosing allergic disease
The incidence of allergy and asthma in both developed and developing nations
is on the rise. According to WHO statistics for the year 2000, asthma
afflicts 100 to 150 million people worldwide, and causes more than 180,000
deaths each year.6 The economic burden of the condition exceeds that of
tuberculosis and HIV/AIDS combined.7 In the US, allergy is the sixth leading
cause of chronic disease, and costs to the healthcare system total $18
billion per year; allergic diseases afflict an estimated 50 million Americans;
and allergic rhinitis accounted for 14 million doctor's office visits
in 2002.8 In Europe, allergy sufferers number 80 million.9
Although
allergy is a common cause of disease, the less serious manifestations
(such as allergic rhinitis) have not always been viewed as requiring the
effort necessary to arrive at a proper diagnosis. But the progression
of allergic disease is better understood today. If at one time the general
perception of allergy was that it was a common but relatively minor nuisance,
it must no longer be regarded as such. There is need to recognize it early
and intervene to prevent progression to more serious allergic manifestations.
With 3gAllergy, a convenient tool is now available to the primary care
physician and the clinical laboratory to improve the quality of allergic
patients' care. By correctly identifying the underlying allergens that
are responsible for allergic disease and its symptoms, the physician can
be alerted to strive to halt the progress of the allergy march; to address
a variety of allergic conditions appropriately; and to maintain patients
below their symptomatic allergic threshold.
The
allergy march
Atopic
dermatitis
Atopic dermatitis (AD) may present at any age, but usually appears in
infancy and is one of the most common skin disorders seen in infants and
children. It is often the first manifestation of the allergy march, which
proceeds from AD to allergic rhinitis and asthma. The allergy march illustrates
the point that IgE-mediated allergic disease often advances in a predictable
manner. Clinical symptoms correspond to age, with eczema found in infants
and young children, followed by gastrointestinal manifestations and, during
preteen and teenage years, by respiratory conditions such as asthma. Children
with atopic dermatitis and a positive family history of atopy have a 40
percent risk of developing asthma.10
One
airway, one disease
It has been suggested that rhinitis and asthma are two manifestations
of one syndrome.11 Rhinitis, which is at least three times as common as
asthma, is documented in 85 to 95 percent of patients with asthma, provided
an adequate history is taken;11 and studies have demonstrated that allergic
rhinitis increases a patient's risk of developing asthma.12
Allergic
rhinitis (AR) may be seasonal or perennial. Seasonal AR is also known
as hay fever, while perennial AR is also known as rhinoconjunctivitis.
Aeroallergens such as pollens and molds in spring, summer and/or early
fall are usually the cause of seasonal AR. Seasonal AR is strongly associated
with sinusitis, otitis media, nasal polyps, sleep apnea and asthma. Perennial
AR symptoms are year-round and are generally related to house dust mites,
animal hair or dander, and mold spores. Some patients may suffer from
both seasonal and perennial AR. In these patients, the low-level monitoring
of allergen-specific IgE, which is possible with 3gAllergy, affords the
physician an opportunity to adopt the best treatment protocol for the
patient.
Asthma
is a chronic disease in which the bronchial tubes of the lungs are chronically
inflamed and the muscles around these tubes tighten to constrict the airways.
Acute inflammation of airways occurs as a result of exposure to aeroallergens
or other asthma triggers such as stress; smoke; certain smells such as
perfumes; activities such as sports; weather conditions such as dry wind
or cold air; and respiratory infections such as sinus infections, flu
and throat infections.
Asthma
may be developed at any age, but it is routinely diagnosed in children
younger than age 5 and in adults in their thirties. Fifty percent of adults
with asthma suffer from allergic asthma; the number for children is close
to 80 percent.13 That allergic asthma is a highly morbid manifestation
of the allergy march, and costly to treat, underscores the need to intervene
during the early manifestations of allergic disease to avert progression
to this stage.
Food
allergies
Although
food allergies may affect people of all ages, they are more frequent in
children. It is important to differentiate a food allergy from a food
intolerance. Any food can act as an allergen and result in sensitization,
but in children the following six foods are responsible for 90 percent
of food allergy reactions: milk, peanuts, soy, egg, wheat and tree nuts
(pecans, walnuts, etc.). The same list, with the addition of fish and
crustaceans (shrimp, lobster, etc.), applies for adults.
In
food allergy, patients may experience itching in the mouth; vomiting;
diarrhea or abdominal pain; a drop in blood pressure; and, particularly
in children, atopic dermatitis, eczema and hives. Allergic reactions to
food may develop rapidly into anaphylaxis, a severe, life-threatening
reaction. There is no cure for food allergies.
Patients
who are extremely allergic and who have severe anaphylactic reactions
are not candidates for skin prick testing because of the danger it poses
for them. Nor is skin prick testing possible for patients affected by
eczema or dermatographism. For all of these patients, blood tests such
as 3gAllergy are an excellent clinical diagnostic tool.
Other
allergic conditions
Additional contexts requiring the recognition of an IgE-mediated process
to allow for correct, timely treatment and to prevent serious consequences
include giant papillary conjunctivitis in response to contact lenses;14,15
sensitization to a new allergen in an injected immunotherapy extract;16
drug allergy; and insect venom allergy, in which patients with a severe
reaction to an insect sting may exhibit negative skin prick test results
and low levels of specific IgE detectable only with a sufficiently sensitive
assay.17
Allergic
threshold
A polysensitized patient may have levels of IgE specific to various allergens
that cumulatively are insufficient to precipitate allergic symptoms. Sensitization
to a new allergen, however, or exposure to an additional allergen to which
the patient is already allergic, may easily result in pushing the total
allergen load over a point at which the patient experiences allergy symptoms—the
allergic threshold.18 By performing allergen-specific IgE testing, the
physician can identify offending allergens. 3gAllergy testing offers the
possibility of monitoring the patient's allergen-specific IgE levels at
low levels. Appropriate intervention can control allergy symptoms, interrupt
the allergy march in children and prevent more serious allergic disease
such as asthma.
|
|
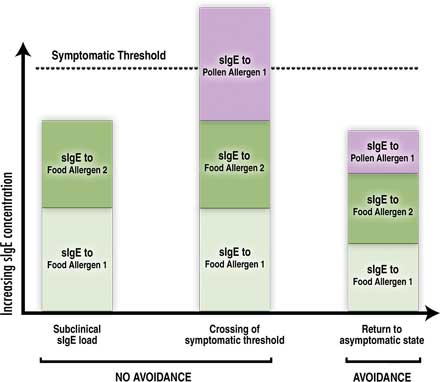
Figure 2. Allergy
is a cumulative threshold disease. (a) In this example, the patient
is allergic to two foods, but the combined contributions of the specific
IgE (sIgE) directed against the two foods is not sufficient for the
manifestation of symptoms. (b) With the addition of a pollen allergen
and in the absence of an avoidance protocol for any of the three allergens,
the patient's cumulative sIgE concentration exceeds the threshold
value and symptoms appear. (c) With the observance of an avoidance
protocol, the patient's cumulative sIgE concentration drops below
the threshold level and the patient's symptoms are under control.
|
Conclusion
Today, the primary care physician must confirm a diagnosis of allergy
and decide whether the patient can receive the appropriate treatment and
necessary follow-up visits or must be referred to an allergy specialist
for care. In this context, 3gAllergy is a valuable diagnostic tool to
assist the primary care doctor with this decision. It is reasonable to
expect that in vitro allergen-specific IgE methods such as 3gAllergy can
lower costs associated with treatment and management of patients who may
suffer from allergic diseases, reduce inappropriate referrals to specialists,
improve the quality of patient care, and help prevent progression to more
morbid disease.
| References |
| 1. |
Wood
RA, Phipatanakul W, Hamilton RG, Eggleston PA. A comparison of skin
prick tests, intradermal skin tests, and RASTs in the diagnosis of
cat allergy. J Allergy Clin Immunol 1999;103(5 Pt 1):773-9. |
| 2. |
Poon
AW, Goodman CS, Rubin RJ. In vitro and skin testing for allergy: comparable
clinical utility and costs. Am J Manag Care 1998;4:969-85. |
| 3. |
Szeinbach
S, Boye M, Muntendam P, et al. Diagnostic assessment and resource
utilization in patients prescribed non-sedating antihistamines. Paper
presented at the Annual Meeting of the American College of Osteopathic
Family Physicians; March 2001; Philadelphia, PA. |
| 4. |
Various
presentations and posters reporting on results with specific IgE testing
on DPC's IMMULITE® 2000 platform are reproduced in Diagnostic Products
Corporation (DPC). Proceedings of DPC's International Conference on
Allergy; 2003 June 6; Paris, France. Los Angeles: The Corporation;
2003. (Document no. ZB214). |
| 5. |
Li
TM, Chuang T, Tse S, Hovanec-Burns D, El Shami AS. Development and
validation of a third generation allergen-specific IgE assay on the
continuous random access IMMULITE 2000 analyzer. Ann Clin Lab Sci
2004;34:67-74. |
| 6. |
World
Allergy Organization. Global Statistics: Allergy Facts. www.worldallergy.org/media/globalstatistics.shtml. |
| 7. |
World
Health Organization. Bronchial asthma: The scale of the problem. www.who.int/mediacentre/factsheets/fs206/en/. |
| 8. |
American
Academy of Allergy, Asthma and Immunology (AAAAI). The Allergy
Report: Science Based Findings on the Diagnosis & Treatment of Allergic
Disorders , 1996-2001. Available at www.niaid.nih.gov/factsheets/allergystat.htm. |
| 9. |
European
Federation of Pharmaceutical Industries and Associations. Disease
burden in Europe. www.efpia.org/2_indust/diseaseburden.htm |
| 10. |
Sasai
K, Furukawa S, Muto T, Baba M, Yabuta K, Fukuwatari Y. Early detection
of specific IgE antibody against house dust mite in children at risk
of allergic disease. J Pediatr 1996;128:834-40. |
| 11. |
Togias
A. Rhinitis and asthma: evidence for respiratory system integration.
J Allergy Clin Immunol 2003;111:1171-83. |
| 12. |
Rachelefsky
GS. National guidelines needed to manage rhinitis and prevent complications.
Ann Allergy Asthma Immunol 1999;82:296-305. |
| 13. |
American Academy
of Allergy, Asthma & Immunology. Pediatric asthma: promoting best
practice. www.aaaai.org/members/resources/initiatives/pediatricasthmaguidelines
/03_NaturalHistory.pdf
and
Asthma and Allergy
Foundation of America. Do you live in an asthma capital? www.aafa.org/display.cfm?id=7&sub=92&cont=461
|
| 14. |
Donshik
PC, Ballow M. Tear immunoglobulins in giant papillary conjunctivitis
induced by contact lenses. Am J Ophthalmol 1983;96:460-6. |
| 15. |
Allansmith
MR: Giant papillary conjunctivitis. J Am Optom Assoc 1990;61(6 Suppl):S42-6. |
| 16. |
Moverare
R, Elfman L, Vesterinen E, Metso T, Haahtela T. Development of new
IgE specificities to allergenic components in birch pollen extract
during specific immunotherapy studied with immunoblotting and Pharmacia
CAP System. Allergy 2002;57:423-30. |
| 17. |
Hamilton
RG, Wisenauer JA, Golden DB, Valentine MD, Adkinson NF Jr. Selection
of Hymenoptera venoms for immunotherapy on the basis of patient's
IgE antibody cross-reactivity. J Allergy Clin Immunol 1993;92:651-9. |
| 18. |
Boner
AL, Peroni DG, Piacentini GL, Venge P. Influence of allergen avoidance
at high altitude on serum markers of eosinophil activation in children
with allergic asthma. Clin Exp Allergy 1993;23:1021-6. |
|