|
|
|||||||
|
Serum Trypsin-like Immunoreactivity (TLI) in Cats and Dogs Diseases of the pancreas are increasingly recognized in cats and dogs. The most common include inflammation of the pancreas (pancreatitis) and exocrine pancreatic insufficiency (EPI), a condition of reduced pancreatic function that results in digestive malabsorption. Conventional diagnostic approaches for both EPI (assay of digestive enzyme activity in feces) and pancreatitis (assay of serum amylase and lipase activities, abdominal radiography, and ultrasonography) offer limited sensitivity and specificity. Studies indicate, however, that trypsin-like immunoreactivity (TLI), a pancreas-specific enzyme, demonstrates high clinical sensitivity and specificity for the detection of EPI in both cats and dogs. In addition, although no single specific test currently exists for pancreatitis in these animals, TLI may assist in its evaluation when used in conjunction with other diagnostic tests. TLI
assays EPI
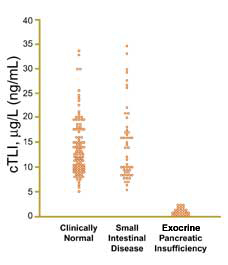
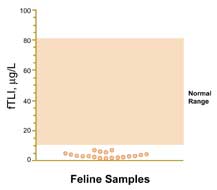
Loss of functional exocrine pancreatic tissue leading to clinical signs of EPI is accompanied by markedly decreased concentrations of serum TLI. Radioimmunossay of TLI in canine serum (cTLI) has proved to be a remarkably specific and sensitive test for EPI since its introduction approximately two decades ago (Figure 1). The relatively recent development of an assay for TLI in feline serum (fTLI) has allowed increased recognition of EPI in cats (Figure 2), a diagnosis that was formerly difficult to make. TLI is now considered the test of choice for EPI in both dogs and cats. It is recommended that serum cobalamin and folate also be assayed in any patient with signs suggestive of EPI, since results of these tests may reveal concurrent or alternative intestinal disease, and correction of vitamin deficiencies may be required for an optimal response to digestive enzyme replacement therapy.
Pancreatitis
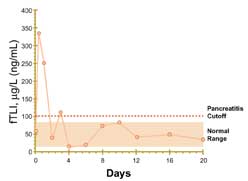
Serum TLI concentrations may be increased in association with pancreatitis for various reasons. Experimental studies have shown that serum TLI concentrations increase rapidly after induction of acute pancreatitis in dogs and cats, sometimes reaching values far greater than 20 times the upper limit seen in healthy animals. The half-lives of trypsinogen and trypsin in plasma are short, however (less than 20 minutes), and values return to those of healthy controls relatively quickly, sometimes within 3 to 4 days (Figure 3). In some patients, transient subnormal values are seen during recovery from acute disease. Diagnostically, elevated values are most commonly noted shortly after onset of clinical signs, after which diagnostic sensitivity may not be as great. Trypsinogen is cleared from the blood fairly rapidly by glomerular filtration. Conse-quently, if renal function is compromised, serum TLI may increase. It is interesting to note in such cases that cats display a much lower threshold for TLI fluctuations than dogs. Whereas serum canine TLI remains essentially static unless severe renal impairment exists, elevations in serum feline TLI occur with only moderately compromised renal function. Available data, however, indicate that serum creatinine values must be highly elevated (greater than 5 mg/L in dogs and 4 mg/L in cats) for significant increases in serum TLI to occur (2- to 3-fold above the upper limit of the reference range). Interpreting
TLI test results and sample handling
While
the half-life of TLI in the blood circulation is rather short (less than
20 minutes), it is very stable in serum and plasma for up to 7 days of
unrefrigerated storage. Serum TLI is unaffected by prolonged freezing
at Conclusion
DPC will soon release canine TLI (cTLI) and feline TLI (fTLI) assays on the IMMULITE® family of systems. Contact your DPC representative for more information on these upcoming assays. Other DPC veterinary assays include double-antibody assays for cTLI and fTLI, buprenorphine (for horses), rat corticosterone, canine total T3, canine total T4 and canine TSH.
|
||||||||
| Home
- Search
- Site
Map - Contact
Us About DPC - Medical Conditions - Technology - Immunoassay Products - Financial - Employment |