|
Growth
Hormone and Related Growth Factor Measurements:
Increasing Demand with Diverse Clinical Applications
by
Michael J. Bennett, Ph.D., FRCPath, FACB
Professor of Pathology and Pediatrics
University of Texas Southwestern Medical Center at Dallas
Director of Clinical Chemistry
Children's Medical Center of Dallas, TX, US
The measurement of human growth hormone (GH) in serum has been useful
for many years in the clinical evaluation of short stature and growth
failure in children due to gross pituitary failure and isolated GH deficiency.
In adults and older children, the measurement of GH has been valuable
for the diagnosis of acromegaly, an abnormal growth acceleration usually
due to pituitary adenomas (tumors), which secrete excessive amounts of
GH.
Although
the clinical measurement of GH has been a standard practice for some time,
the mechanisms of action and regulation have not been fully defined. Increasingly,
interactions of GH with its target hormones, previously known as somatomedins
but now referred to as insulin-like growth factors (IGFs), and its inhibitory
element, somatostatin, have been implicated in a wide array of disease
states including somatic growth defects and cancer.
This
overview will focus specifically upon the interactions and pathophysiology
of GH and IGF-I and will address the clinical importance of measuring
these components in serum.
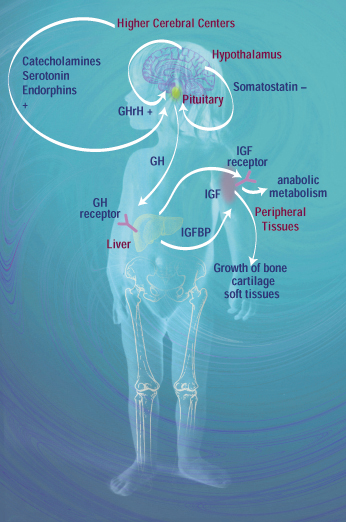
GH
is a polypeptide (191 amino acids) secreted from the somatotrope cells
of the anterior pituitary in response to various stimuli. These stimuli
include the hypothalamic release of a polypeptide (40 amino acids) called
growth hormone-releasing hormone (GHrH). Release of GH is also modulated
by higher centers in the brain. Stimuli such as stress and hypoglycemia,
which result in increased catecholamine production, also promote GH release
into the circulation (Figure 1). GH release by the pituitary is inhibited
by the action of somatostatin, otherwise known as growth hormone-inhibiting
hormone, a hypothalamic peptide (14 amino acids) that also has an inhibitory
effect on TSH secretion by the anterior pituitary, and on insulin and
glucagon secretion by the pancreas.
| Figure
1. Physiological control of GH, IGF and IGFBP production and release. |
|
|
The
overall effect of GH is to promote growth of bone and cartilage and to
promote anabolic (growth) pathways in all tissues. The effects are mediated
by IGFs, with IGF-I being quantitatively the most significant of these
growth factors. The polypeptides IGF-I (17 kDa) and IGF-II (22 kDa) are
alternately spliced products of a single gene located on chromosome 12q22-q24.1.
They are synthesized by the liver in response to GH stimulation via a
GH receptor. IGFs are transported in the circulation by members of a family
of GH-dependent IGF-binding glycoproteins, of which insulin-like growth
factor binding protein-3 (IGFBP-3) is the most significant. IGFBP-3 is
responsible for the transport of 75 percent of circulating IGF-I. IGFs
have structures that are remarkably similar to insulin, but they have
far greater growth properties. Their mechanism of action is through cell
membrane receptors that are similar to insulin receptors.
Clinical
utility of GH measurement
GH levels fluctuate considerably under baseline conditions, as they depend
upon many factors. Consequently, random samples may lead to erroneous
conclusions in cases of both hypersecretion and deficiency. A number of
inhibition/stimulation tests have been devised to better determine GH
status.
Hypersecretion
of GH
Individuals with acromegaly or pituitary gigantism due to pituitary adenoma
typically demonstrate a flat GH response to an oral glucose load, whereas
normal individuals demonstrate GH levels that fall to less than 2 ng/mL,
30 to 60 minutes after an oral glucose load.
Hyposecretion
of GH
Diagnosing growth hormone deficiency in children who are failing to grow
at the normal rate is crucial. Pediatric endocrinologists must often distinguish
short children who are truly GH deficient and will achieve their expected
growth potential through expensive GH therapy from children who are constitutively
short and will not realize therapeutic benefits. It is also very important
to identify children with a GH deficiency before epiphyseal fusion of
the long bones takes place, as treatment is unlikely to be effective after
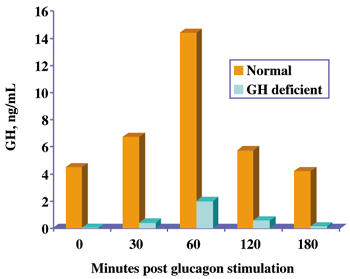
this time. Random GH levels are generally uninformative and a number of
stimulation tests have been devised to test GH reserves. These include
insulin-induced hypoglycemia or glucagon stimulation. A peak GH level
in excess of 10 ng/mL is regarded a a normal response whereas a peak level
below 10 ng/mL is generally regarded as a case of GH deficiency (Figure
2).
|
Figure
2. Normal and deficient responses during a glucagon stimulation
test for GH deficiency.
|
|
|
The
pathophysiological nature of the GH deficiency must be identified, as
this will assist in determining the appropriate treatment regimen. Organic
deficiency of GH, due to isolated failure of the pituitary to secrete
GH or other pituitary hormones (panhypopituitarism), generally responds
well to GH therapy. In the case of panhypopituitarism, other aspects of
the endocrine system need to be investigated including the thyroid, gonadotropic
and adrenocortical axes. Nonorganic causes of GH deficiency include malnutrition
and psychosocial deficiency due to poor social contact. These causes may
be reversible without the need for GH therapy if the adverse conditions
are addressed.
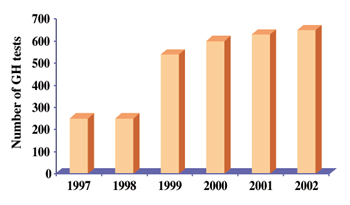
Experience
of performing in-house GH measurement in a tertiary care pediatric center
Prior to the introduction of an in-house service for GH measurement in
Children's Medical Center (CMC) of Dallas, Texas, samples were sent out
to a reference laboratory with a concomitant delay in turnaround. In 1999,
the CMC introduced a chemiluminescence-based GH assay and in-house service
(initially IMMULITE®, currently IMMULITE® 2000).
Most of the requests for GH measurement have been for the evaluation of
short stature. This requires a glucagon stimulation test that is performed
in the clinic, with samples being collected at 0, 30, 60, 120 and 180
minutes. The five samples are analyzed sequentially upon receipt of the
180-minute sample in the laboratory and results are reported within minutes.
The CMC endocrinologists are now able to act immediately, as results often
become available while the patient is still in the clinic. This improved
turnaround has resulted in an impressive increase in orders for this test
(Figure 3).
| Figure
3. Increase in the number of orders for GH testing at Children's Medical
Center in Dallas after the 1999 introduction of in-house service using
the IMMULITE®,
and later, the IMMULITE® 2000 system. |
|
|
Measurement
of IGF-I and IGFBP-3 in the clinical laboratory
Both IGF-I and IGFBP-3 secretion are dependent upon the pituitary release
of GH. In the cases of hyper- and hyposecretion of GH, the result is an
increase or decrease in the hepatic synthesis or release of IGF-I and
IGFBP-3. While there is still only a relatively small amount of data on
the utility of IGFBP-3 measurement, it has been suggested that measurement
of IGF-I is superior to that of GH in evaluating both acromegaly and GH
deficiency states. IGF-I levels do not appear to fluctuate as much as
GH, although other endocrine disorders may also result in low IGF-I levels.
The increased availability of sensitive assays for these important growth
factors will provide the opportunity to evaluate the best determinants
of abnormal growth.
Mutations
in the IGF gene
A number of mutations in the IGF gene have been described, which result
in severe growth retardation in the homozygous-deficient state. Carriers
for these mutations also tend to be short in stature, suggesting a possible
heterozygous gene dose effect, which may potentially be a very important
determinant of growth in a larger population. Paradoxically, the homozygous-affected
individuals tend to have high GH levels, as do patients who have mutations
in the GH receptor, so that even high GH levels may eventually provide
clues to the etiology of short stature.
IGF-I
and cancer
High circulating IGF-I levels have been implicated in prostate growth,
hyperplasia and malignancy. Prostate-specific antigen (PSA) is still the
most powerful independent predictor of prostate cancer, but adding IGF-I
to the receiver operator curve for PSA has been shown to improve the predictive
value of PSA measurement. Other studies have shown a strong relationship
between circulating IGF-I concentrations and breast cancer in premenopausal
but not postmenopausal women. Clearly, further studies on the role of
IGF-I and cancer could provide critical insights into the mechanisms of
oncogenesis.
Conclusion
Serum GH measurements have demonstrated long-standing utility in the clinical
evaluation of specific growth abnormalities. Inhibition/stimulation tests
are generally more valuable than basal determinations, as GH levels are
in constant flux. Related growth factors such as IGF-I and IGFBP-3, synthesized
in response to GH secretion, exhibit more stable plasma levels. Many investigators
have indicated that IGF measurements may actually provide more useful
information than those of GH in the evaluation of acromegaly and GH deficiency
states. In addition, high IGF-I serum levels may be strongly predictive
of risk for a variety of malignancies. Currently, the clinical issues
surrounding GH are generating more questions than answers. It is hoped
that further research will eventually lead to a more conclusive body of
evidence in this area.

|